Chief complaint: left-sided pleuritic pain for 1 year
Medical history: unremarkable
Physical examination and laboratory findings: unremarkable
Initial Clinical Approach
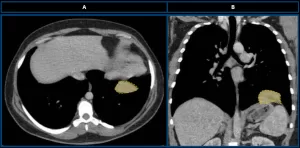
Chest computed tomography (CT) performed in the Netherlands
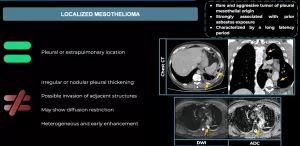
Axial (A) and coronal (B) CT scans (mediastinal window) demonstrate a solid, well-defined, homogeneous lesion with soft-tissue density (yellow dotted line) located at the base of the left hemithorax.
Initial Differential Diagnosis
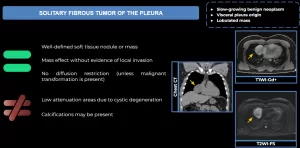
SOLITARY FIBROUS TUMOR OF THE PLEURA
LOCALIZED MESOTHELIOMA
PERIPHERAL LUNG ADENOCARCINOMA
Chest MRI
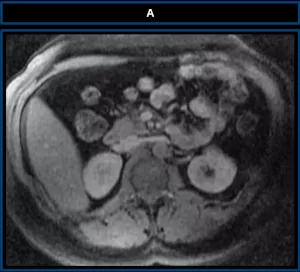
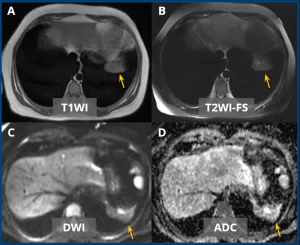
Axial MRI images in T1-weighted (A), T2-weighted with fat suppression (B), DWI (C), and ADC (D) sequences demonstrate a lesion with elongated/discoid morphology, centered at the base of the left hemithorax (yellow arrows), demonstrating isointense signal on T1, mildly hypointense signal on T2, and no diffusion restriction.
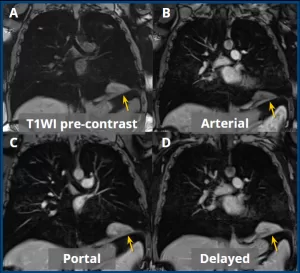
Pre-contrast (A) and post-contrast T1-weighted sequences in the arterial (B), portal venous (C), and delayed (D) phases, all with fat suppression, demonstrate slow and progressive enhancement after contrast administration (yellow arrows).
Post-MRI Differential Diagnoses
In this case, the main differential diagnoses should include:
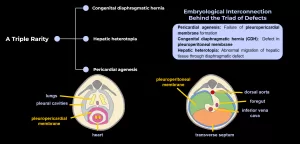
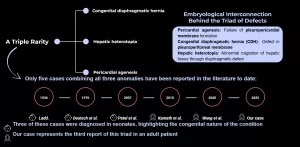
Hepatic Heterotopia Associated With Congenital Diaphragmatic Hernia And Pericardial AgenesisLara Carolina Peixoto Quiche, MDRadiology and Diagnostic Imaging ResidentOrientador: Dr. Eduardo Kaiser Urahy Nunes Fonseca, MDInstituição: Einstein Hospital Israelita
Congenital Absence of the Left Pericardium
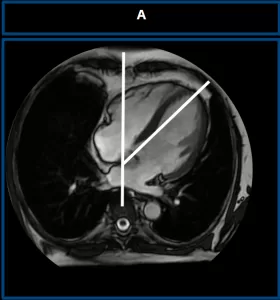
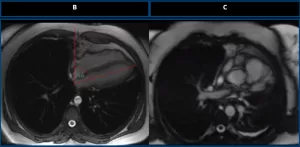
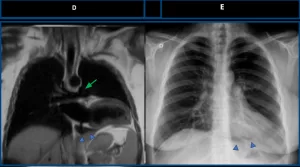
Axial chest MRI of a healthy control (A) demonstrates normal cardiac rotation. A vertical reference line is drawn along the spine. The cardiac axis forms an angle of less than 60° indicating normal positioning.Axial T1-weighted MRI (B) shows excessive clockwise rotation of the heart, with a cardiac axis angle greater than 60°, a characteristic finding of left pericardial agenesis. Axial T2-weighted MRI (C) confirms the abnormal cardiac orientation, supporting the diagnosis.Coronal T2-weighted MRI (D) demonstrates interposition of lung tissue in the aortopulmonary window (green arrow), as well as lung interposed between the diaphragm and the cardiac base (blue arrowheads). Frontal chest radiograph (E) also shows lung interposition between the diaphragm and the inferior cardiac border (blue arrowheads), consistent with left pericardial agenesis.
Hepatic Heterotopia
Types of Hepatic Heterotopia (Collan et al.)
Type I: Accessory liver lobe with a vascular pedicle
Type II: Small accessory lobe attached directly to the liver
Type III: Ectopic liver with no connection to the native liver
Type IV: Microscopic ectopic liver tissue (incidental finding)
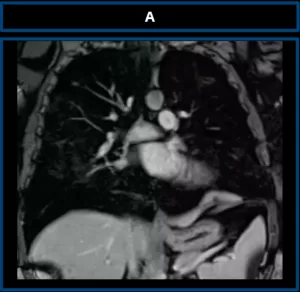
Coronal T1-weighted post-contrast MRI (A) shows a well-defined mass at the base of the left hemithorax with imaging features identical to native liver, including signal intensity and enhancement pattern — supporting the diagnosis of hepatic heterotopia.
Our case corresponds to Type I — a pedunculated accessory lobe herniated into the thoracic cavity through a congenital diaphragmatic defect.
Case Outcome
Postoperative chest MRI Postoperative axial T1-weighted MRI (A) demonstrating successful resection of the ectopic hepatic lesion previously located at the base of the left hemithorax.The patient experienced complete resolution of symptoms and no further complaints following surgical resection and definitive diagnosisDespite its benign nature, the diagnosis was clinically significant: histopathology revealed that the ectopic liver tissue was already cirrhotic, representing a potential precursor to hepatocellular carcinoma (HCC) if left undetected.
References
Wang X, Chen H, Yang L, Lu C. Adult congenital diaphragmatic hernia with absent pericardium and liver heterotopia. Eur J Cardiothorac Surg. 2020;58(4):867–9.
Kamath GS, Borkar S, Chauhan A, Chidanand B, Kashyap N, Warrier R. A rare case of congenital diaphragmatic hernia with ectopic liver and absent pericardium. Ann Thorac Surg. 2010;89(5):e36–7.
Patel Y, McNally J, Ramani P. Left congenital diaphragmatic hernia, absent pericardium, and liver heterotopia: a case report and review. J Pediatr Surg. 2007;42(5):e29–31.
Deutsch AA, Brown KN, Freeman NV, Stanley DA. A case of diaphragmatic hernia, absent pericardium, and hamartoma of liver. Br J Surg. 1972;59(2):156–8.
Cardinale L, Ardissone F, Garetto I, Marci V, Volpicelli G, Solitro F, et al. Imaging of benign solitary fibrous tumor of the pleura: a pictorial essay. Rare Tumors. 2010;2(1):e1.
Ladd WE. Congenital absence of the pericardium. N Engl J Med. 1936;214(5):183–7.
Bak SH, Kim C, Kim CH, Ohno Y, Lee HY. Magnetic resonance imaging for lung cancer: a state-of-the-art review. Precis Future Med. 2022;6(1):49–77. doi:10.23838/pfm.2021.00170.
Collan Y, Hakkiluoto A, Hästbacka J. Ectopic liver. Ann Chir Gynaecol. 1978;67(1):27–9. PMID: 637502.


 Coronal T1-weighted post-contrast MRI (A) shows a well-defined mass at the base of the left hemithorax with imaging features identical to native liver, including signal intensity and enhancement pattern — supporting the diagnosis of hepatic heterotopia.
Our case corresponds to Type I — a pedunculated accessory lobe herniated into the thoracic cavity through a congenital diaphragmatic defect.
Coronal T1-weighted post-contrast MRI (A) shows a well-defined mass at the base of the left hemithorax with imaging features identical to native liver, including signal intensity and enhancement pattern — supporting the diagnosis of hepatic heterotopia.
Our case corresponds to Type I — a pedunculated accessory lobe herniated into the thoracic cavity through a congenital diaphragmatic defect.